ARTICLE ORIGINAL
SILVA, Fábio Tenório [1], FECURY, Amanda Alves [2], UTZIG, Ingrid Lara de Araújo [3], OLIVEIRA, Euzébio [4], DENDASCK, Carla Viana [5], DIAS, Claudio Alberto Gellis de Mattos [6]
SILVA, Fábio Tenório. Et al. Number of confirmed cases of tuberculosis in Brazil between 2007 and 2016. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 05, Ed. 04, Vol. 04, pp. 94-104. April 2020. ISSN:2448-0959, Access link in: https://www.nucleodoconhecimento.com.br/health/cases-of-tuberculosis, DOI: 10.32749/nucleodoconhecimento.com.br/health/cases-of-tuberculosis
ABSTRACT
Tuberculosis is an infectious disease caused by the bacterium Mycobacterium tuberculosis. According to the World Health Organization (WHO), Asia and Africa are the continents with the largest number of confirmed cases on the planet. The objective of this study was to show the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016. The research was conducted in DATASUS database and in scientific articles. The results show that the number of confirmed cases of the disease remained stable for nine years, presenting a sharp drop in the last year of the study; the southeastern region had the highest number of confirmed cases, followed by the northeast of the country, south, north and midwest, respectively; people in the age group between 20 and 59 years presented the largest number of cases; the male gender is approximately twice more affected by tuberculosis than the female; and pulmonary tuberculosis had much higher numbers than the extrapulmonary form and the cases of people with both types of the disease. Agglomeration of people facilitates the spread of M. tuberculosis bacteria. The number of cases of pulmonary tuberculosis was greater than the number of extrapulmonary cases because it is airborne rapidly in environments with many people. Adult individuals appear to be more susceptible to tuberculosis, as there is no vaccination campaign for this age group. However, the chances of cure are higher when using the correct treatment. Apparently, there was an improvement in the organization of health in Brazil and a better preparation of the health professionals in tuberculosis care.
Keywords: Tuberculosis, classification, epidemiology.
INTRODUCTION
Tuberculosis is an infectious disease caused by the bacterium Mycobacterium tuberculosis. According to the WHO, Asia and Africa are the continents with the highest number of confirmed cases on the planet (Mjid et al., 2015).
Smoking and some infections such as HIV, for example, increase the chances of developing tuberculosis and, even though it is not a hereditary disease, the family environment is a great facilitator to the transmission. Thus, extra care should be taken in homes where someone is infected (Mjid et al., 2015).
Tuberculosis is transmitted by contact between people by airway through contaminated droplets. The risk of acquiring the disease is defined by the degree of approximation of infected individuals. Despite numerous strategies adopted by WHO to eradicate it, several factors influence (such as immigration and population individualism, for example). In collective settings, it is necessary to isolate infected persons, specially in hospitals (Abouda et al., 2014).
There are two types of tuberculosis: pulmonary (TB) and extrapulmonary (TBE), and there may be cases of people with both types. The difference between them is the location of their development. TB has its concentration and development in the lungs. TBE has the development of bacteria in other parts of the body (Daronco et al., 2012; Mjid et al., 2015).
The symptoms of TB and TBE can be associated or not. People infected with TB may have a cough for more than three weeks, night sweats, fever, lack of appetite, chest pains, and weight loss. The symptoms of TBE depend on where M. tuberculosis is installed. When the bacterium inhabits the pulmonary pleura, for example, in addition to the symptoms presented in pulmonary tuberculosis, there is a lack of air and chest pain (Daronco et al., 2012).
The diagnosis of TBE is more complicated than TB due to the lower number of bacteria that this disease presents. The methods developed to diagnose are: radiography of the chest to identify lesions in the lung; blood test to see if the white blood cells are producing larger amounts of proteins that damage the replication of bacteria; and the Xpert MTB/RIF test, a modern method based on the evaluation of the bacteria’s presence from the patient’s sputum collection and incubation (Abouda et al., 2014; Daronco et al., 2012).
The treatment of tuberculosis occurs from medicines that attack Mycobacterium tuberculosis. It must be daily, during fasting by the morning. WHO has declared four effective remedies for the treatment of the disease in the initial phase: isoniazid, rifampicine, pyrazinamide and ethambutol. The first part of the treatment usually lasts four months and must be accompanied by the doctor responsible to avoid complications (Dhahri et al., 2014).
The second phase of treatment is made with the antituberculins like isoniazid and rifampicine. This part lasts according to the clinical situation of the patient. The remedies can have side effects like high fever and abdominal pains. In case of such effects, it is necessary to identify what drug is causing them and stop the treatment immediately (Dhahri et al., 2014).
The prevention of tuberculosis occurs from childhood, with the application of the CGB vaccine (Calmette-Guérin Bacillus) in children at the end of the first year of life. This vaccine has a reliability of 60% to 90% and it seems to contribute to a decrease in the mortality and worsening of tuberculosis transmission (Abouda et al., 2014).
According to a survey conducted in 2015 by the SINAN/MS, the number of new cases of tuberculosis in Brazil up to September 2014 was equal to 50,781. In 2015 the northern region of the country presented approximately 6,376 cases; the southeastern region had approximately 29,024 cases; the northeastern region had approximately 16,294 confirmed cases. According to the Ministry of Health, the south region had 2,211 cases and the midwest region presented 2,256 cases of tuberculosis (Barcelar et al., 2014; Chaves et al., 2017).
AIM
The aim of this study is to show the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016.
METHODOLOGY
This research was carried out in the database DATASUS (http://datasus.saude.gov.br/). Connecting the “Access to Information” tab, the option “Health Information (TABNET)” was selected and the option “Epidemiological and Morbidity” was clicked. After the link to the new page, we chose “Cases of Tuberculosis – 2011”. The “Tuberculosis – from 2011” alternative was elected, and the “Brazil by region, state and municipality” filter was selected under “Geographic coverage”. Then, in the new opened window, “Confirmed Cases” were considered under Content, and in Column, the “Not active” option was evaluated for all Line types that were subsequently selected. For each preference, the data of each year were collected between the period from 2009 to 2016 in the “Periods available” area. The Lines used were “Diagnostic Year”, “Gender”, “Form”, “Entry Type”, “Age Range” and “Notification Region”.
This research was done within the Excel application, component of the Microsoft Office suite. Bibliographical research was carried out in books and scientific articles, in the library of the Federal Institute of Education, Science and Technology of Amapa, Campus Macapa, located at: Highway BR 210 KM 3, zip code: 68.909-398, Macapa, Amapa, Brazil
RESULTS AND DISCUSSION
Figure 1 describes the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016. The data show that the number of cases remained stable for nine years, showing a sharp drop in the last year of the study.
Figure 1 Number of confirmed cases of tuberculosis in Brazil between the years 2007 and 2016.
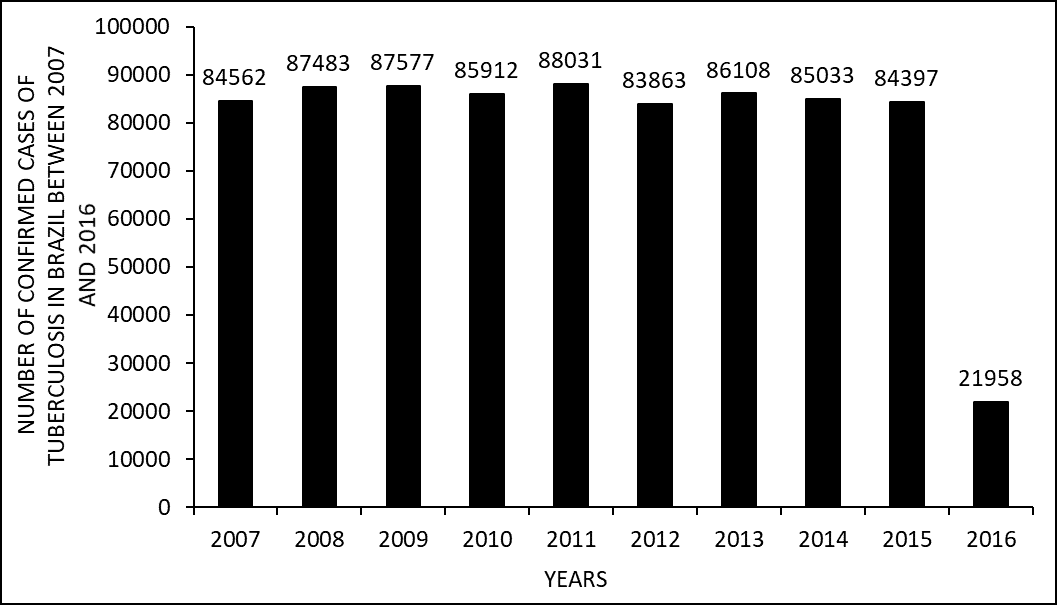
This fact may be related to the improvement in the brazilian health organization and the improvement of health professionals’ training in tuberculosis care. The method of diagnosis made from the evaluation of the patient’s sputum also seems to influence this decline, since it is the fastest methodology in the identification of the bacterium (Cozer et al., 2016; Mehiri-Zeghal., 2015).
Figure 2 shows the number of confirmed cases of tuberculosis between 2007 and 2016 divided by regions of Brazil. It is noted that the Southeast region has the highest number of confirmed cases, followed by the northeast of the country, south, north and midwest, respectively.
Figure 2 Number of confirmed cases of tuberculosis between 2007 and 2016 by regions of Brazil.

This may have occurred due to population geographic factors. As tuberculosis is a disease transmitted by proximity, so crowding of people would facilitate its spread. Data from the last census of the Brazilian Institute of Geography and Statistics (IBGE) indicate that the Southeast has the largest population among Brazilian regions, followed by the Northeast, South, North and Midwest. This is the same order of incidence in the regions of the country found in this research (Abouda et al., 2014).
Figure 3 shows the number of confirmed cases of tuberculosis by age group in Brazil between 2007 and 2016. Data prove that the largest number of cases occur in the age group between 20 and 59 years old.
Figure 3 Number of confirmed cases of tuberculosis by age group in Brazil between 2007 and 2016.
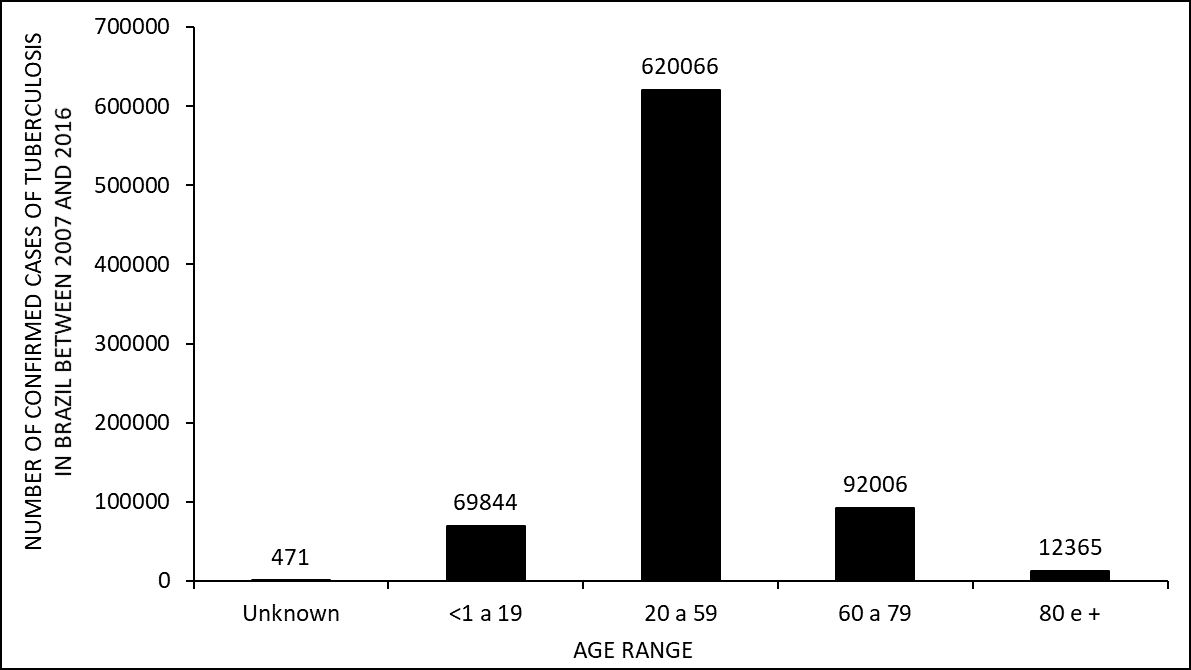
The duration of the CGB vaccine protection would be about 15 years. As the CGB vaccine is given to children, adult people appear to be more susceptible to tuberculosis, as there is no vaccination campaign for this age group. According to the IBGE (2012), the life expectancy of the Brazilian is 74.6 years old, therefore the group of individuals over 80 years old presents a smaller number of cases, possibly because they are smaller in the population (Abiteboul et al., 2010).
Figure 4 shows the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016, divided per gender. The research presents data indicating that male are approximately twofold affected by tuberculosis than female.
Figure 4 Number of confirmed cases of tuberculosis in Brazil by gender between 2007 and 2016.
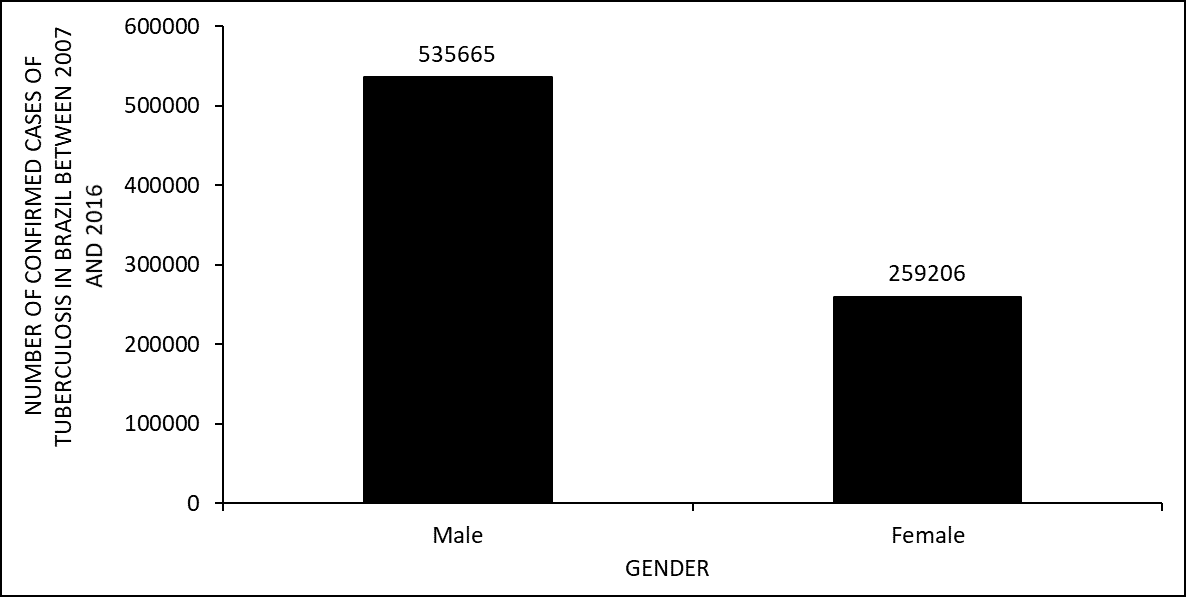
Men’s lack of health care probably explains this. Unlike women, they do not deal with primary health care normally controlled through routine visits to health facilities. This conception is generated by cultural aspects (Gomes et al., 2011).
Figure 5 explains the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016 by the form of the disease. The cases confirmed with TB are much higher than the other two types. Cases of TBE appear in much lower number along with the number of both forms at the same time.
Figure 5 Number of confirmed cases of tuberculosis in Brazil between 2007 and 2016 due to the form of the disease.
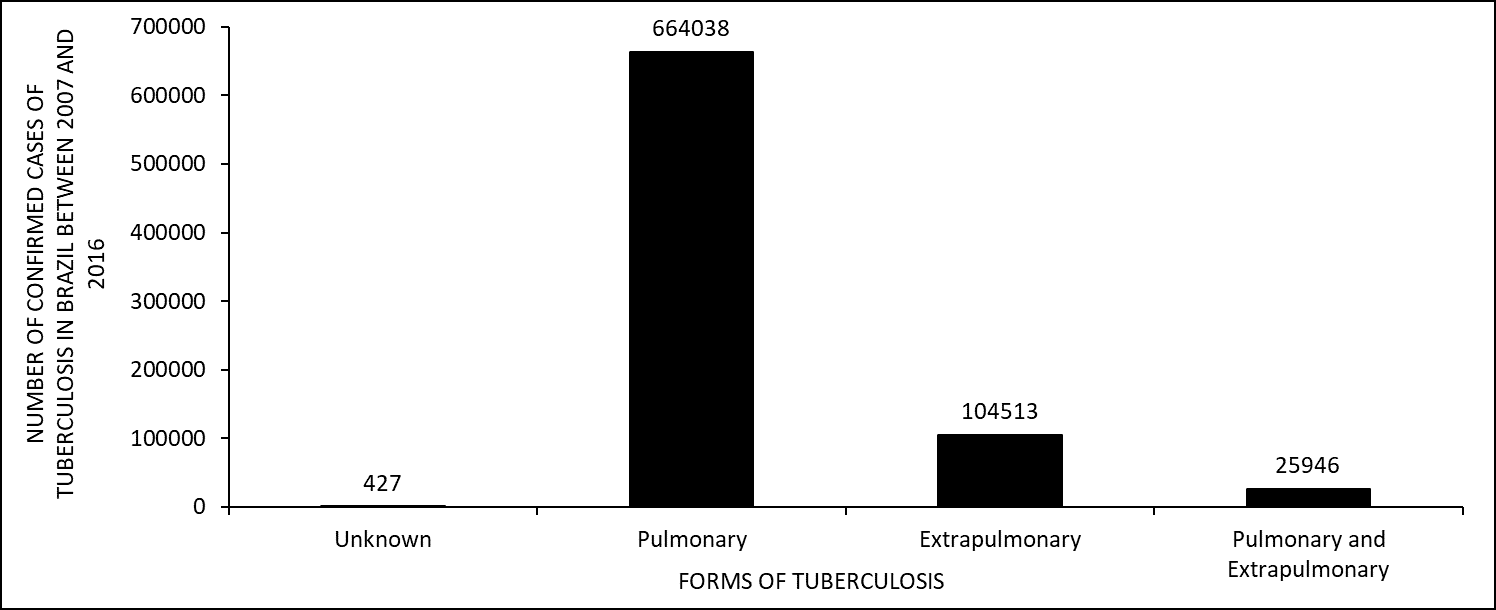
The literature agrees with these results, because TB appears to be quickly transmitted through the air in environments with many people. What may explain the smallest number of cases of TBE is its form of propagation. The bacteria needs to enter the body from the inspiration and move to different organs, other than the lungs. This may require longer time and stimulates a greater immune response (Cozer et al., 2016; Dhahri et al., 2014).
Figure 6 shows the number of confirmed cases of tuberculosis in Brazil between 2007 and 2016, divided by type of entry. The graph indicates that new cases have a greater number than the number of cases of the other types of entry.
Figure 6 Number of confirmed tuberculosis cases in Brazil between 2007 and 2016 by type of entry

A possible reason for this would be the high chances of cure using the correct treatment. This appears to occur with the majority of people infected with Mycobacterium tuberculosis (Daronco et al., 2012; Orofino et al., 2012).
CONCLUSION
Agglomeration of people facilitates the spread of Mycobacterium tuberculosis bacteria. The number of cases of pulmonary tuberculosis was greater than the number of cases of the extrapulmonary type because it is quickly transmitted through the air in environments with many people. Adult individuals appear to be more susceptible to tuberculosis, as there is no vaccination campaign for this age group. However, the chances of cure are higher when using the correct treatment. Apparently, there was an improvement in the organization of health in Brazil and a better preparation of the health professionals in tuberculosis care.
REFERENCES
ABITEBOUL, D.; FLORET, D.; AUTRAN, B.; BEYTOUT, J.; COLOMBAN, B.; DUFOUR, V.; LÉVY-BRUHL, D.; JACQUET, A.; JARLIER, V.; MALADRY, P.; NICAND, E.; PATY, M.-C.; POIRIER, C. Pertinence du maintien de l’oligation de vaccination par le BCG des professionnels listés aux articles L3112-1, R.3112-1 et R.3112-2 du code de la santé publique. Haut Conseil de Santé Publique, 2010.
ABOUDA, M.; YANGUI, F.; TRIKI, M.; KAMMOUN, H.; KHOUANI, H.; CHARFI, M.R. Prévention de la tuberculose. Elsevier Masson SAS, v. 71, p. 159-167, 2014.
BARCELAR, A.; FRAGA, A. C. P.; Lobo, A. P.; PELISSARI, D. M.; OLIVEIRA, P. B. Panorama da tuberculose no Brasil – Indicadores epidemiológicos e operacionais. Ministério da Saúde, v. 01, p. 57-71, 2014.
BEN AMAR, J.; Dhahri, B.; AOUINA, H.; AZZABI, S.; BACCAR, M. A.; EL GHARBI, L.; BOUACHA, H. Traitement de la tuberculose. Elsevier Masson SAS, v.71, p.122-129, 2014.
CHAVES, J.; TOMILIN, B. A.; BRUN, D.; Fuhr, L. G.; OURIQUE, F.; PILLETTI, K.; KRUMMENAUER, M. L.; PEIXOTO, S. L.; FERNANDES, R.; FREITAS, A. L.; PORCIÚNCULA, A. S.; RODRIGUES, M. T. Perfil dos pacientes com tuberculose que foram atendidos em uma unidade de referência do município de Santa Cruz do Sul – RS no período de 2009 a 2013. J. Health Sci., v. 05, p. 31-36, 2017.
COZER, A. M.; ASSIS, L. P. F.; GRACIANO, A. R.; AMÂNCIO, V.; DIAS, D. C. S. Panorama da tuberculose no Brasil. Rev. Educ. Saúde, v. 04, p. 43-50, 2016.
DARONCO, A.; SONDA, E. C.; SILVEIRA, C. S.; BEE, G. R.; PASSOS, P.; BORGES, T. S.; POSSUELO, L. G.; CARNEIRO, M. Aspectos relevantes sobre tuberculose para profissionais de saúde. Rev Epidemiol Control Infect, v. 02, p. 61-65, 2012.
GOMES, R.; MOREIRA, M. C. N.; NASCIMENTO, E. F.; REBELLO, L. E. F. S.; COUTO, M. T.; SCHRAIBER, L. B. Os homesn não vêm! Ausência e/ou invisibilidade masculina na atenção primária. Ciência e Saúde Coletiva, v. 16, p. 983-992, 2011.
IBGE. Expectativa de vida. Disponível em: <https://teen.ibge.gov.br/noticias-teen/7827-expectativa-de-vida>. Acessado no dia 19 de setembro de 2017.
IBGE; DOU. População Estimada. Disponível em: <ftp://ftp.ibge.gov.br/Estimativas_de_Populacao/Estimativas_2014/estimativa_dou_2014.pd>. Acessado no dia 12 de setembro de 2017.
MJID, M.; CHERIF, J.; BEN SALAH, N.; TOUJANI, S.; OUAHCHI, Y.; ZAKHAMA, H.; LOUZIR, B.; MEHIRI-BEN RHOUMA, N.; BEJI, M. Épidémiologie de la Tuberculose. Elsevier Masson SAS, v. 71, p. 67-72, 2015.
OROFINO, R. L.; BRASIL, P. M. A.; TRAJMAN, A.; SCHMALTZ, C. A. S.; DALCOLMO, M.; ROLLA, V. C. Preditores dos desfechos do tratamento da tuberculose. J Bras Pneumol, v. 38, p. 88-97, 2012.
SLIM-SAIDI, L.; MEHIRI-ZEGHAL, E.; GHARIANI, A.; TRITAR, F. Nouvelles méthodes de diagnostic de la tuberculose. Elsevier Masson SAS, v. 71, p. 110-121, 2015.
[1] Mining technician by the Institute of Basic, Technical and Technological Education of Amapá (IFAP).
[2] Biomedical, PhD in Topical Diseases, Professor and researcher of the Medicine Course at Campus Macapá, Federal University of Amapá (UNIFAP).
[3] Degree in Letters / English, Fellowship in English Language, Teacher and researcher at the Institute of Basic, Technical and Technological Education of Amapá (IFAP).
[4] Biologist, PhD in Topical Diseases, Professor and researcher of the Physical Education Course at, Federal University of Pará (UFPA).
[5] Theologian, PhD in Psychoanalysis, researcher at the Center for Research and Advanced Studies – CEPA.
[6] Biologist, PhD in Theory and Research of Behavior, Professor and researcher of the Chemistry Degree Course at the Basic, Technical and Technological Institute of Amapá (IFAP).
Submitted: April, 2020.
Approved: April, 2020.















